NORMAL:
- DURA: The dura is fixed at the foramen magnum and C1/2 and inferiorly at the coccyx. In between the dura is suspended in the canal and held in place by the spinal roots and fine connective tissue thickenings (Hoffman's Ligaments) in the epidural space.
- FLEXION: With flexion there is stretching of the posterior dura but no significant movement.
HIRAYAMA DISEASE:
- DURA: It is thought that in Hirayama Disease, dura does not grow in length to the same degree as the spinal column in adolesence and is taut in the neutral position.
- FLEXION: With flexion there is no ability for the taut dura to stretch, resulting excessive anterior movement of the posterior dura. This displaces the cord anteriorly which repeatedly indents against the vertebral bodies with resultant ischaemia of the anterior cord (anterior horn cells).
MRI findings in Hirayama disease are:
NEUTRAL SCANS:
- Increased anterior cord T2 signal at the lower cervical level.
- +/- Anterior cord atrophy at the same level.
FLEXION SCANS:
- Anterior movement of the posterior dura.
- Anterior displacement of the cord with flattening/ obliteration of the anterior CSF space.
- Widening of the posterior epidural space with enhancement of the epidural fat post contrast.
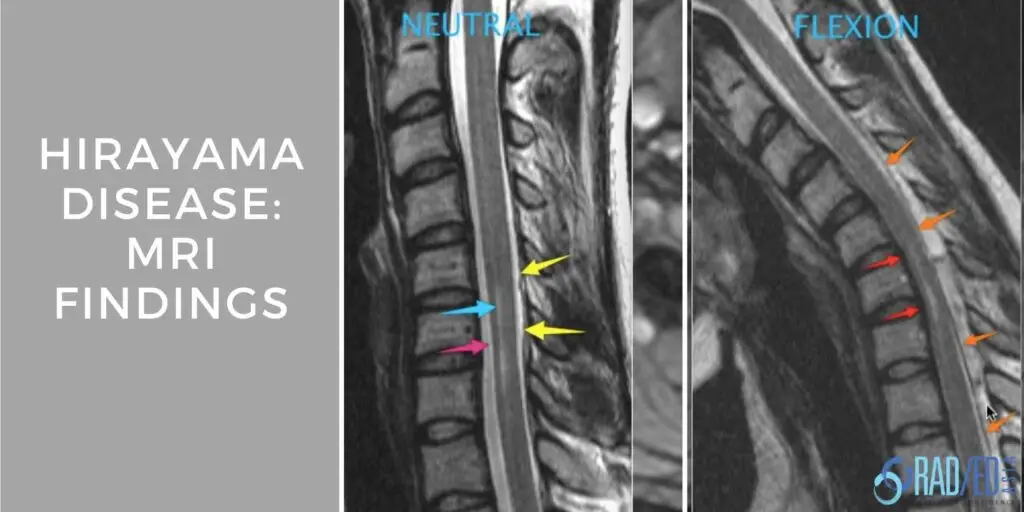
 Image Above: Neutral: Increased T2 signal in the anterior cord (blue arrow) with slight atrophy of the anterior margin of the cord (pink arrow). The dura (yellow arrow) is in a normal position. Flexion: Posterior dura has moved anteriorly (orange arrows) and cord is displaced against the posterior vertebral margin with loss of the anterior CSF (red arrows). With contrast (not shown) there is intense enhancement of the posterior epidural space in epidural veins.
Image Above: Neutral: Increased T2 signal in the anterior cord (blue arrow) with slight atrophy of the anterior margin of the cord (pink arrow). The dura (yellow arrow) is in a normal position. Flexion: Posterior dura has moved anteriorly (orange arrows) and cord is displaced against the posterior vertebral margin with loss of the anterior CSF (red arrows). With contrast (not shown) there is intense enhancement of the posterior epidural space in epidural veins. As flexion views are not routinely performed, how do you suspect Hirayama Disease on a routine Cervical MRI and then bring the patient back to do flexion scans?
- Appropriate clinical information of asymmetric upper limb muscle weakness in an adolescent/ young male together with,
- Increased cord signal +/- anterior cord atrophy at the lower cervical level with no apparent cause such as a disc or osteophyte.
Jakhere S, Wagh V. Hirayama's disease: The importance of flexion magnetic resonance imaging. J Postgrad Med 2011;57:48-50.
Monali Raval et al Indian Journal of Radiology and Imaging / November 2010 / Vol 20 / Issue 4.
V.T. Lehman et al Cervical Spine MR Imaging Findings of Patients with Hirayama Disease in North America: A Multisite Study AJNR Am J Neuroradiol 34:451–56 Feb 2013.
Kimmell et al Spinal dural attachments to the vertebral column: An anatomic report and review of the literature Surg Neurol Int. 2011; 2: 97.



