Gleno Humeral Ligaments

Learn how to identify the Middle Glenohumeral Ligament (MGHL) on shoulder MRI scans and differentiate it from labral tears.
![]()
Identifying the gleno humeral ligaments on MRI can be challenging as they are small and on lower field strength scanners there is inadequate resolution to see them properly.
However, if we understand the anatomy of the ligaments, it becomes easier to know where to look even if we can’t directly identify the ligament. This is the 2nd in the series (First post on the Superior Gleno Humeral Ligament click on this link SGHL
This post is an adaptation of a talk given at Radiology Asia in Singapore titled Gleno Humeral Ligaments made Easy…er.
![]()

There are 3 main Glenohumeral ligaments.
1. SGHL: Superior GlenoHumeral Ligament (Click here for more on the SGHL )
2. MGHL: Middle GlenoHumeral Ligament
3. IGHL: Inferior GlenoHumeral Ligament
4. The Coraco Humeral Ligament (CHL) is extra capsular and is not part of the Glenohumeral ligaments, but we will also look at as it helps to identify the SGHL and it also fuses with the joint capsule at the rotator interval. (Click here for more on the CHL)![]()
The ligaments arise in an orderly fashion and using analogies often helps to understand anatomy. On sagittal scans the ligaments have the appearance of tentacles of an octopus radiating from the biceps insertion on the supra glenoid tubercle.
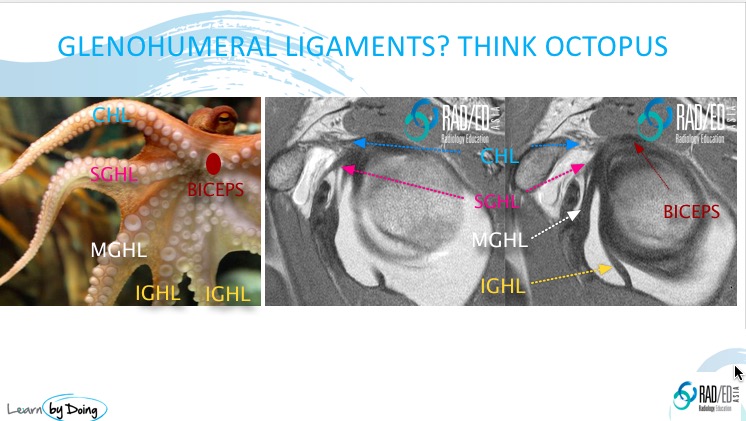
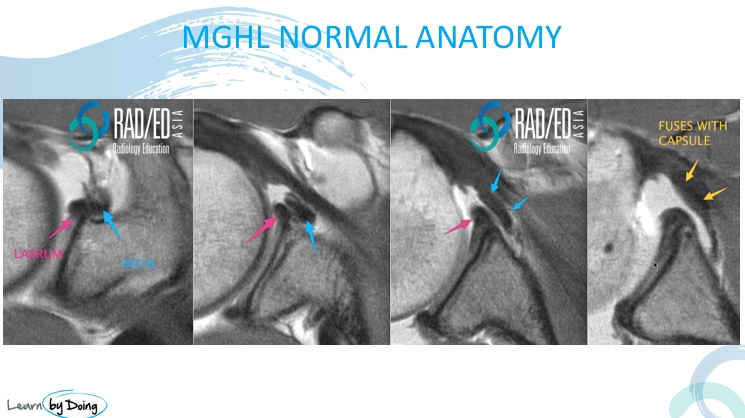
After having identified the CHL (Blue arrow) and SGHL (Pink arrow), the next structure that you see immediately below it on sagittal scans is the MGHL (White arrow).
![]()
![]()
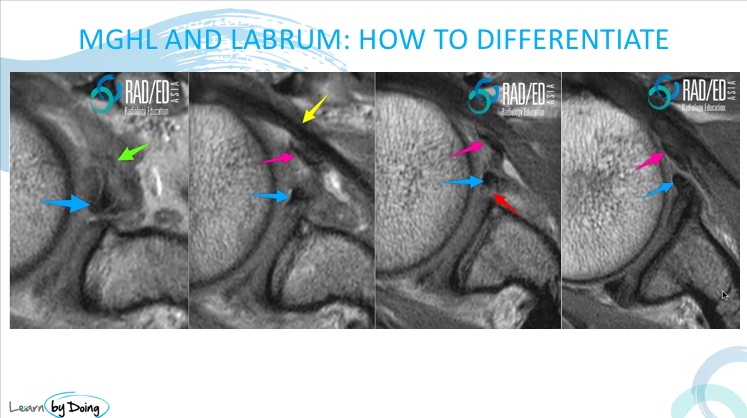
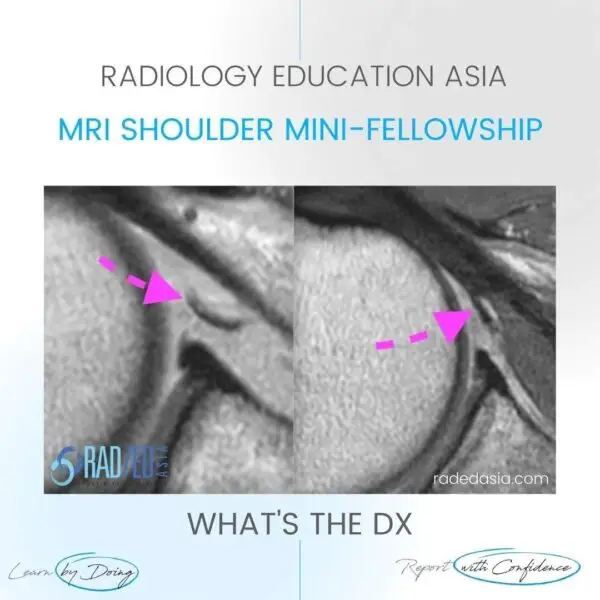
Image above: Two black, linear structures. Which is the labrum, and which is the MGHL?
![]()
Read Article “The Middle Glenohumeral Ligament: Normal Anatomy, Variants & Pathology” from Springer Nature Link, Read HERE
![]()
Labrum.![]()
Subscapularis.![]()
CHL.![]()