Spondylolytic myelopathy and Myelomalacia
Spondylolytic myelopathy and Myelomalacia are quite different but there is often confusion between the use of the terms. Let’s look at what they are and how to differentiate them.
![]()
SPONDOLYTIC MYELOPATHY
Refers to increased T2 signal in the cord, from oedema, due to extrinsic compression of the cord (degenerative causes like disc, osteophyte) which is symptomatic. But it is potentially reversible if the extrinsic compression is relieved, and the patient’s symptoms might improve.
MYELOMALACIA
Refers to increased T2 signal in the cord, BUT the cord is atrophic and gliotic as a result of a chronic injury of any form and is irreversible and the patient’s symptoms will not improve.
These terms are often confused because both conditions result in high T2 signal in the cord and reduced cord size. But the implications of each diagnosis are very different.
SO HOW DO WE DIFFERENTIATE THE TWO?
Is there extrinsic compression of the cord at/ around the level of the high T2 signal in the cord?
If there is, this is spondylotic myelopathy and the patient may benefit from decompression.

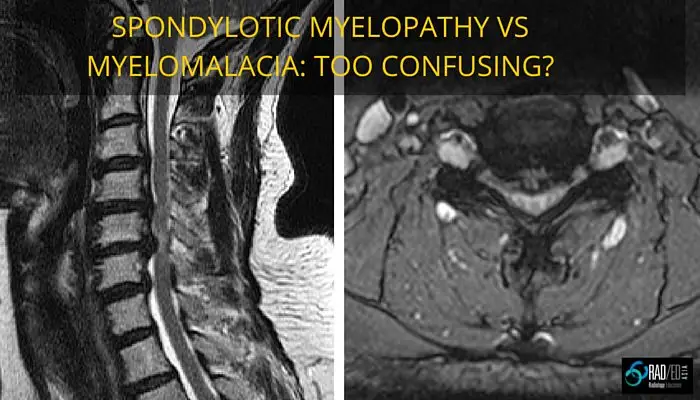
Images above: First image: Arrow at region of cord oedema with adjacent extrinsic compression. Second Image: Arrow at disc causing cord compression and cord oedema.
If there is is no extrinsic compression and the cord is small and bright, this is myelomalacia which is cord atrophy and gliosis. The patient will not benefit from any surgery.

Image above: Arrows at regions of increased cord signal, the cord is small and no extrinsic compression (Post laminectomy).
CAN SPONDYLOTIC MYELOPATHY AND MYELOMALACIA CO EXIST?
Yes. But at the initial time of imaging, when there is extrinsic compression, you cant differentiate the two, as both are high signal on T2 and can coexist. So when you see a compressed cord with high T2 signal, there may be potentially reversible cord oedema (myelopathy) and atrophy (myelomalacia) present together. The patient has to be decompressed and rescanned a few months later, only then will you know if there is any atrophy. Cord oedema that was initially present from the compression should have resolved and any residual T2 high signal will now be due to atrophy (myelomalacia).

Inital scan shows extrinsic cord compression, increased T2 signal and a small cord = Spondylotic Myelopathy +/- unknown amount of myelomalacia. Post decompression: Extrinsic compression relieved, cord has expanded slightly BUT residual T2 cord signal = residual myelomalacia.