This site is intended for Medical Professions only. Use of this site is governed by our Terms of Service and Privacy Statement which can be found by clicking on the links. Please accept before proceeding to the website.
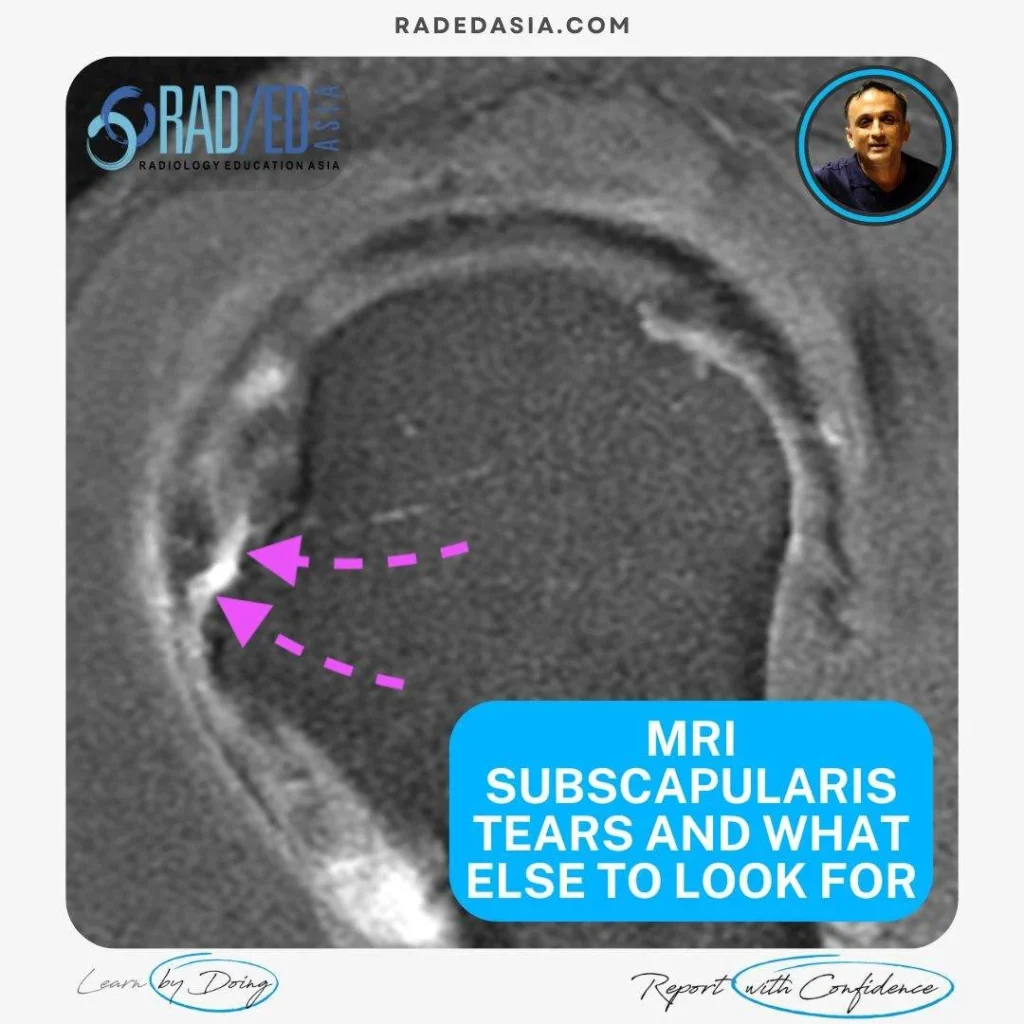
MRI Assessment of the subscapularis tendon is not just about looking for tears. This post looks at the four things that should be assessed.
![]()
![]()
![]()
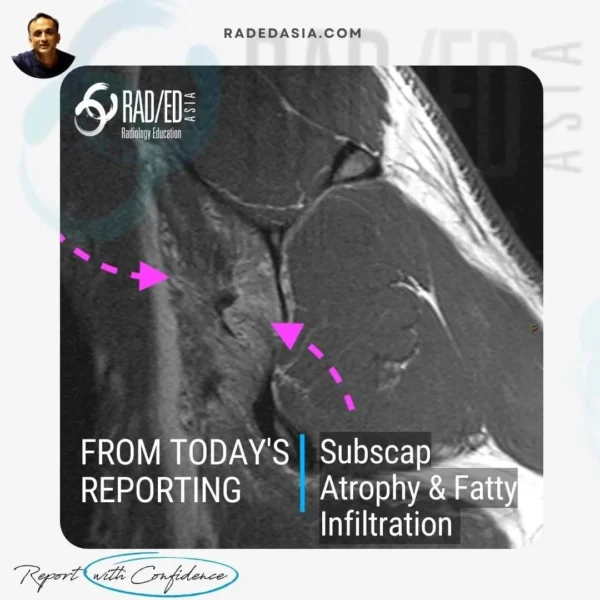
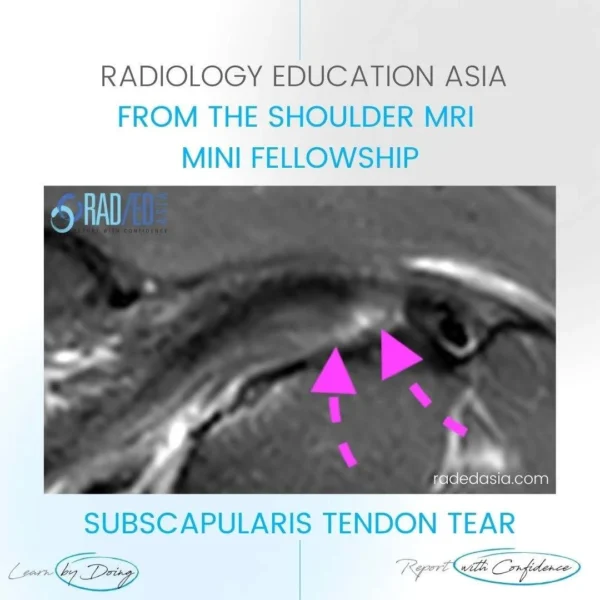
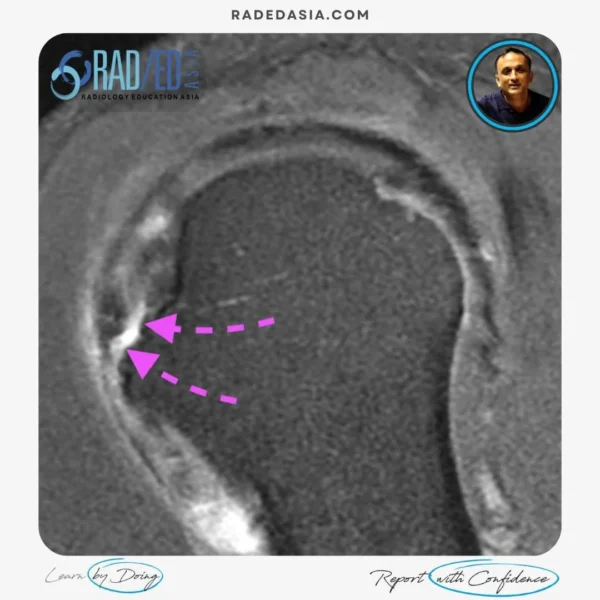
Muscle atrophy and fatty infiltration are two important findings to look for in any rotator cuff tendon tear.
![]()

![]()
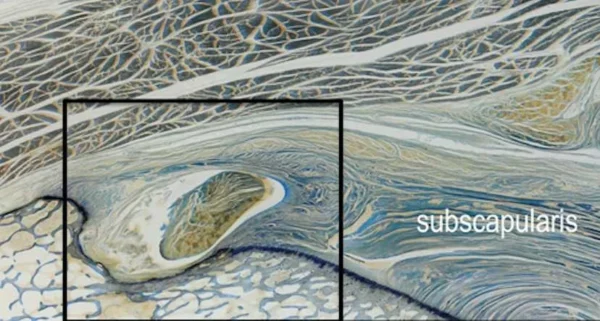
Image from: Tamborrini G et al. The Rotator Interval Ultrasound Int Open 2017; 3: E107–E116.![]()


