RHEUMATOLOGY

MRI SPINAL CORD COMPRESSION. MRI LEPTOMENINGEAL DISEASE ENHANCEMENT
When you get a referral for a patient with KNOWN carcinoma for ” MRI? cord compression”, when do you give contrast?
There is a wide variation in when contrast is given for patients who come in with known malignancy and neurological symptoms. Often, contrast is not given when it is required.
Take a fairly common request. “Patient has breast cancer. New lower limb neurology? Spinal cord compression”
The usual routine would be to do a Sagittal T1 and T2 of the region of concern and
![]()
If you see a cause for the patient’s symptoms such as a pathological fracture compressing the cord the most important thing to then do is a screening T2 scan of the entire spine, as there may be multiple sites of compression that also require treatment.
Contrast can then be given to completely exclude leptomeningeal lesions.
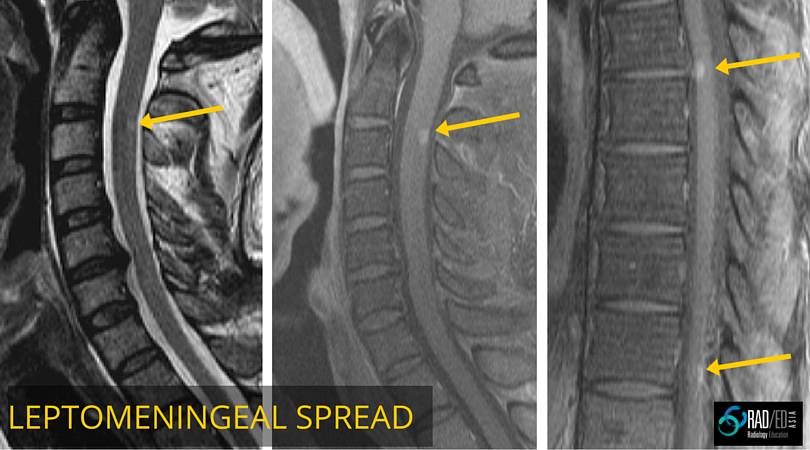
Image above: Breast carcinoma. Faint T2 signal posterior C2/3. Post contrast enhancement of leptomeningeal metastasis at C2/3 and at thoracic cord not seen on non contrast scans.
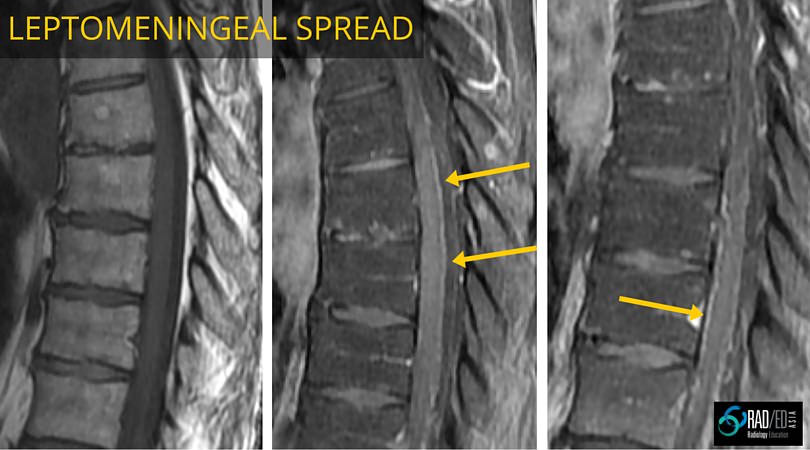
Image above: Breast carcinoma leptomeningeal metastases. First image T1 non con no abnormality. Subsequent two images post contrast leptomeningeal sugar coating of cord from metastases.
![]()